The gold standard for removing mercury
About the author:
Graeme Munro-Hall

Holistic dentist Graeme Munro-Hall shares his protocol for removing your amalgam fillings safely
I started life as a conventional drill, fill and bill dentist. This meant working with amalgam and gold, and doing exactly as I was taught in dental school. It was patch-and-repair dentistry with little intrinsic satisfaction to it.
In my late 20s, I was at an American Dental Association (ADA) conference in the US where I was offered a cardiac check-up. Ten minutes after my measurements had been taken, I was in front of the nurse who, glancing at the data, told me to see the cardiac specialist in the neighbouring booth now. I was the only one selected for this out of a long line of far more elderly dentists than myself.
The cardiologist examined the electrocardiogram, listened to my heart and gave me a blood test. When the blood test came back, it showed massively high levels of 'bad' cholesterols, predisposing factors for a large, probably fatal, heart attack. Furthermore, all these indications were a sign of stress on the heart and that I needed to do something about it urgently, although he could not suggest exactly what should or could be done.
As I later discovered, my problems were entirely due to mercury from dental amalgam. As well as having amalgam and gold fillings myself, I had been using amalgam on a daily basis without any protection since I was a student at dental school. I had my amalgam and other dental metals removed, using a form of the metal-removal protocol we use now on our patients. Although at the time I put myself in the position of an experimental guinea pig, I not only survived the removal, but also felt better. I knew then that we were on to something significant.
The fact that I am here today at over 60 years of age with blood pressure at 125/80 mmHg, blood chemistry the envy of a 30-year-old, no thickening of the arteries, a heart back in its place and a low cholesterol level is wholly the result of all our efforts and research.
The IAOMT protocol
The International Academy of Oral Medicine and Toxicology (IAOMT) has established the recommended minimum treatment protocol for safe removal of dental amalgam. This should be followed whenever amalgam fillings (or other dental metals) are being removed. The point of the protocol below is to minimize the amount of mercury released from the patient and absorbed by the dental staff when drilling out old amalgams.
- The patient breathes a separate air or oxygen supply
- The operator and staff wear mercury-absorbing masks
- The patient wears eye protection
- Amalgams are 'chunked' out, not ground out
- High-speed drills are used with copious amounts of water irrigation and coolant
- The air in the operating room is filtered to remove mercury vapour
- A rubber dam or 'clean-up' tips are used to isolate the teeth during amalgam removal
- The patient's skin and clothing is covered, with only minimal skin exposure
- The mouth is constantly rinsed to remove amalgam particles and mercury vapour
- The patient wears eye protection
- Amalgams are 'chunked' out, not ground out
- High-speed drills are used with copious amounts of water irrigation and coolant
- The air in the operating room is filtered to remove mercury vapour
- A rubber dam or 'clean-up' tips are used to isolate the teeth during amalgam removal
- The patient's skin and clothing is covered, with only minimal skin exposure
- The mouth is constantly rinsed to remove amalgam particles and mercury vapour
- High-speed suction is in use at all times in the mouth.
Failure to observe these rudimentary steps will increase mercury exposure to the patient. Naturally, it also goes without saying that the debris collected (the old amalgam) must be responsibly disposed of to protect the environment. Regulations about waste mercury are rather stringent because it is recognized by various environmental agencies as an extremely hazardous substance.
My additional 'V-Tox' protocols
The V-Tox method described below uses the IAOMT protocol, but goes even further.
- The patient must be prepared by taking the appropriate supplements before fillings are removed.
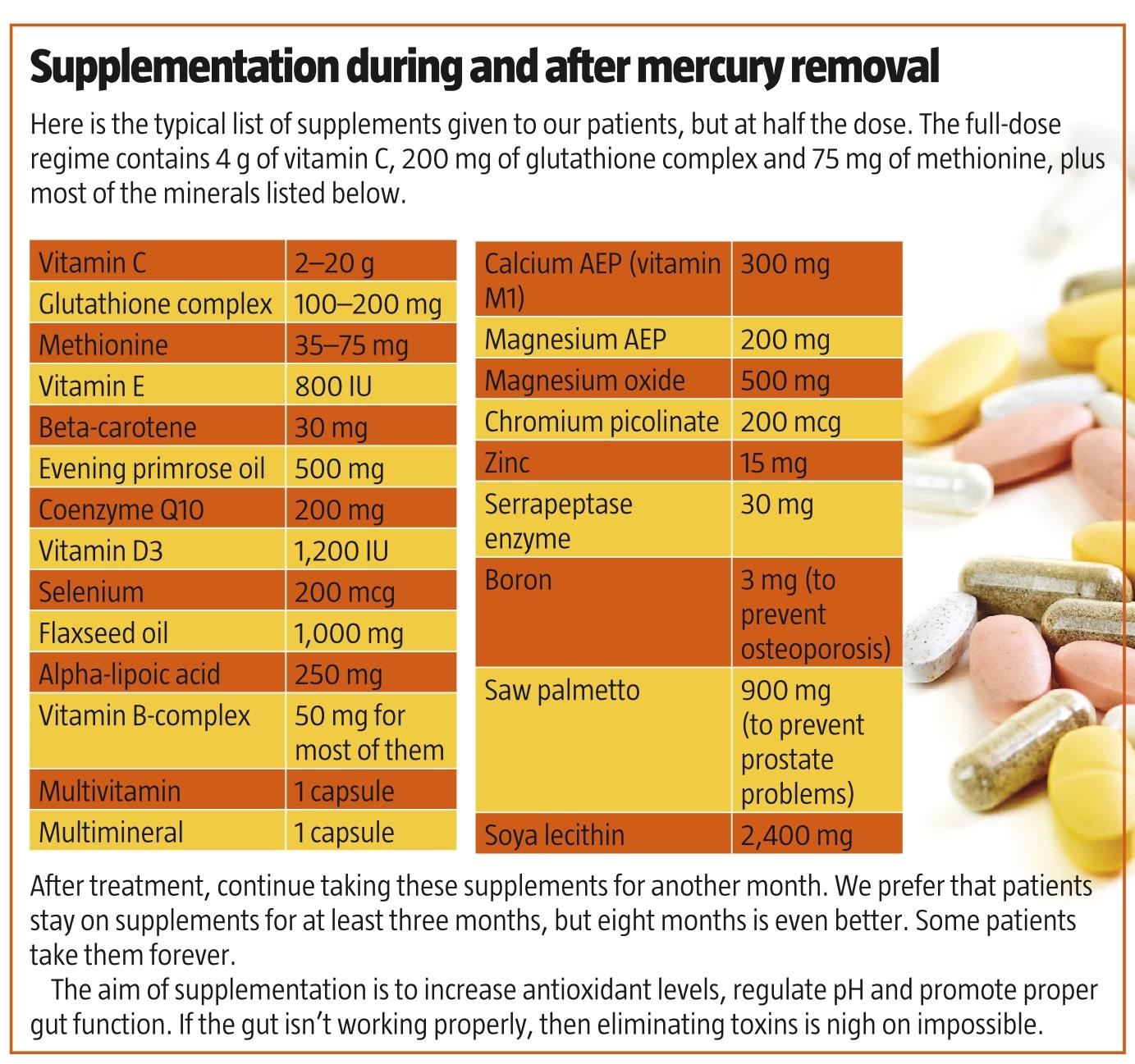
- Intravenous vitamin C with glutathione is administered to the patient during or immediately after metal or amalgam removal for one to four days. The amount of vitamin C depends on the weight and condition of the patient, but a minimum of 0.75 g/kg body weight, diluted in Ringer's (sodium) lactate solution (to replace lost fluids and electrolytes), and 800-1,500 mg of glutathione are used for every infusion. In some cases, two infusions are given daily (see box, page 55). Vitamin C and glutathione bind to mercury and remove it effectively and safely from the body. Indeed, intravenous vitamin C is the cornerstone of my V-Tox therapy.
- Preparation for removal varies a little from patient to patient, but the basic principles are that the patient's blood pH and basal temperature are measured for a week beforehand, then repeated three months after treatment and compared as a measure of progress.
How vitamin C removes mercury
Vitamin C is a reducing agent: it removes metals from the body not by chelation, as do DMPS, DMSA or EDTA, but by oxidation/reduction reactions—similar to what the body does. Chelation, on the other hand, chemically grabs the metals and minerals, and strips them from the body, along with all the essential minerals, such as magnesium and copper. This is the danger of chelating agents, especially with long-term use.
Vitamin C works by donating an electron, which is essentially what antioxidants do. When mercury is bound to tissues, it is forced to accept an electron from vitamin C and, when it does this, the bond is weakened and the metal is released.
Imagine a mercury atom hanging on by one hand like a monkey to a branch in a tree. Along comes vitamin C and gives the monkey a banana (an electron); the monkey makes a grab for the banana, but then falls from the tree. Mercury in this state is less reactive and finds it difficult to rebind itself to tissues.
While in this state, glutathione wraps the mercury up securely and takes it to the colon, where it is excreted. After glutathione does this, it needs to be regenerated so it can wrap up more mercury. Regenerating glutathione also requires an electron from vitamin C. So if enough vitamin C is available, glutathione can keep on regenerating and removing mercury, plus a host of other toxins as well.
In addition, vitamin C rehydrates cells, allowing them to revert back to their proper shape. Cells function properly only when they are the correct shape, as they interact with body messenger hormones through lock-and-key mechanisms on the cell membrane. Vitamin C also powers up mitochondria, the energy providers of cells, allowing the cells to work at a high rate of efficiency.
Oral vitamin C dosages
Vitamin C given orally can cause looseness of the bowels. This is called 'bowel tolerance', and it varies from individual to individual and according to the degree of ill health of the individual. For maintenance of health, far higher doses are required: at least 1,000 mg/day.
On a personal note, I have taken vitamin C daily for nearly 30 years at a dose of 10,000-20,000 mg (10-20 g) to remove mercury and recover from my heart condition, and I have had only positive effects.
Intravenous vitamin C dosages
Vitamin C used intravenously has an entirely different effect. Intravenous vitamin C (IV-C) actually sucks water from the bowel, so instead of producing loose bowels, it has a tendency towards constipation. However, this is mitigated by the thirst patients then experience when receiving IV-C, a thirst that should be satisfied only with good-quality water.
There is a threshold for the amount of IV-C needed for a therapeutic effect: 0.75 g of IV-C per kg of body weight. This is the minimum; under severely toxic conditions, this can go up to 1 g of IV-C per kg of body weight. In patients with severe cavitation or other infections, two infusions of IV-C may be given on the same day. This will speed up the rate of healing enormously, reduce the risk of infection, reduce the chances of postoperative swelling and bruising, and reduce pain.
These high doses are diluted in Ringer's lactate solution to a ratio of one part vitamin C to four parts Ringer's. The IV-C is also buffered to make its pH compatible with that of the patient's blood. Ringer's lactate solution itself contains blood plasma and electrolytes to the same ratio as found in the blood circulation.
This infusion is given at a rate of 72 drops per minute; this means that an average infusion will last between two to three hours. A saline solution may be used instead of Ringer's, but this may cause dizziness and a feeling of disorientation in some patients.
When not to use IV-C
The only contraindication to the use of IV-C is a deficiency of glucose-6-phosphate dehydrogenase (G6PD). However, G6PD is a liver enzyme that is rarely found to be deficient—we ourselves have come across it only twice in more than 20 years. It is found usually, but not always, in people of Eastern Mediterranean or African descent. A simple blood test can determine if G6PD deficiency is present.
Kidney disease or dysfunction is often stated as a contraindication of IV-C use. This is not the case; in fact, the exact opposite is true.
Your treatment programme
- Get a thorough dental examination beforehand
- Have a treatment plan for removing dental metals and infections
- Use supplements to raise antioxidant status and regulate blood pH
- Dental treatment should be carried out over two days
- IV-C should be used at high doses and administered for three to four days, including the days of dental treatment; more infusions may be required
- Maintain a high level of antioxidants and minerals in the body for eight months
- Monitor your progress at three-, eight- and 18-month intervals
- Go for additional therapies if indicated.
The mercury-removal diet
• Eliminate sugar and refined flour completely
• Eat butter and yoghurt, but reduce or eliminate milk
• Increase the number of eggs and good protein
• No alcohol (it's a form of sugar), no caffeine and no undiluted fruit juices
• Drink clean mineral water at a minimum of 1 L/day
• Stick to this diet during the preparation and treatment phase, and mostly keep to it afterwards as well.
Excerpted from Toxic Dentisty Exposed by Graeme Munro-Hall (Browsebooks, 2009)
No comments:
Post a Comment