 Health Benefits of the Natural Squatting Position by JONATHAN ISBIT (Click on author's name to see his PubMed articles) |
 |
|
 |
 Reference: Tagart REB. The Anal Canal and Rectum: Their Varying Relationship and Its Effect on Anal Continence, Diseases of the Colon and Rectum 1966: 9, 449-452. |
 The new device symbolized the "progress" and "creativity" of western civilization. It showed that Man could "improve" on Nature and transcend the primitive cultural practices followed by the poor "benighted" natives in the colonies. The "White Man's Burden" typified the condescending Victorian attitude toward other races and cultures. The British plumbing industry moved quickly to install indoor plumbing and water closets throughout the country. The great benefits of improved sanitation caused people to overlook a major ergonomic blunder: The sitting position makes elimination difficult and incomplete, and forces one to strain. Those who could not overlook this drawback had to keep silent, because the subject was considered unmentionable. Furthermore, how could they criticize the "necessary" used by Queen Victoria herself? (Hers was gold-plated, befitting the self-styled "Empress of India.") So, like the Emperor’s New Clothes, the water closet was tacitly accepted. It was a grudging acceptance, as evidenced by the popularity of "squatting stools" sold in the famous department store, Harrods of London. As shown below on the left, these footstools merely elevated one's feet in a crude attempt to imitate squatting.  Learn more about this comparison 150 years ago, no one could have predicted how this change would affect the health of the population. But today, many physicians blame the modern toilet for the high incidence of a number of serious ailments. Westernized countries have much higher rates of colon and pelvic disease, as illustrated by this report in the Israel Journal of Medical Science: The prevalences of bowel diseases (hemorrhoids, appendicitis, polyps, ulcerative colitis, irritable bowel syndrome, diverticular disease, and colon cancer) are similar in South African whites and in populations of prosperous western countries. Among rural South African blacks with a traditional life style, these diseases are very uncommon or almost unknown.19The following sections will examine these and other diseases in more detail to see how an unnatural toilet posture could produce such a wide range of harmful effects. top of page |
 Pictures of ancient public toilets tend to confuse westerners, who assume that they were used in the sitting position. This impression is often reinforced by the pose of a comical tourist. Pictures of ancient public toilets tend to confuse westerners, who assume that they were used in the sitting position. This impression is often reinforced by the pose of a comical tourist.But, in reality, these are squattoilets. 
The ancient Romans used the posture shown below on the left. (Togas were more convenient than trousers, and provided some degree of privacy.)
  Note: The Sulabh International Museum of Toilets website claims that archeologists have found "sitting-type" toilets at ancient sites, thousands of years old. The author of the site, Dr. Bindeswar Pathak, was asked for his evidence that these toilets were used in the sitting position. He replied that he actually has no evidence, but was simply repeating the assumptions of western archeologists. top of page |
The cecum is a small pouch where the colon begins, in the lower right section of the abdomen. Wastes from the small intestine flow into the cecum through the ileocecal valve (theoretically a one-way valve.) The appendix is a narrow tube attached to the cecum, with a channel opening into the cecum. Waste matter can get lodged in this channel, causing the appendix to become infected and inflamed. Immediate surgery must be performed to remove the appendix before it bursts. Otherwise, the result is usually fatal. Why does the appendix get blocked with fecal matter? Did nature make a blunder in its design? One clue comes from the field of epidemiology. Appendicitis is a disease of westernized countries, virtually unknown in the developing world.19,31 The reason is that the cecum was designed to be squeezed empty by the right thigh, in the squatting position. On a sitting toilet, it is physically impossible to compress the cecum. Instead, one pushes downwards with the diaphragm, while holding one's breath. This maneuver inflates and pressurizes the cecum. It is analogous to squeezing a tube of toothpaste in the middle and causing the bottom of the tube to inflate. The pressure can easily force wastes into the appendix, with disastrous consequences. The back-pressure can also overwhelm the ileocecal valve, whose purpose is to protect the small intestine from fecal contamination. Barium enema exams and intestinal surgeries routinely show the leakage of wastes into the small intestine. Crohn's Disease develops in the area soiled by this toxic backwash. Despite all the straining, the cecum never gets evacuated. Residual wastes adhere to the colon wall, increasing the risk of cancer and inflammation (including appendicitis.) By contrast, in the squatting posture, the right thigh squeezes the cecum from its base. Its contents are thoroughly expelled into the ascending colon, where peristalsis carries them away. There is no need to hold one's breath or push downwards, since the posture generates the pressure automatically. The force is all directed upwards, so the appendix stays clean and the ileocecal valve stays closed. These organs were not "poorly designed" – as is currently taught in medical schools. Like the rest of the colon, they were designed with squatting in mind. Historical Background of Appendicitis The epidemiology of appendicitis poses many unanswered questions. Almost unknown before the 18th century, there was a striking increase in its prevalence from the end of the 19th century, with features suggesting it is a side effect of modern Western life.30In 1886, Reginald Heber Fitz, a Harvard Professor of Pathological Anatomy, became the first doctor to recognize and name the disease. He was also the first one to propose treating it by removing the appendix.18The conservative British medical establishment resisted the novel appendectomy procedure until after the turn of the century, when it was used to save the new king's life. In 1901, the Prince of Wales, Albert Edward, underwent an emergency appendectomy, just two weeks before his scheduled coronation as King Edward VII. His successful recovery finally convinced British surgeons that this operation was the only way to save the victims of this "mysterious" new disease.20 Currently, 7% of the U.S. population will contract appendicitis at some point in their lifetime (according to www.emedicine.com). The figure would be even higher, except that 40,000 "incidental appendectomies" are performed each year (according to Harper's Index, Feb, 2002.) "Incidental" means there was nothing wrong with the appendix, but the surgeon happened to be operating on another organ nearby – in most cases performing a hysterectomy. Appendicitis is the most common reason for a child to need emergency abdominal surgery. Young people between the ages of 11 and 20 are most often affected (according to www.KidsHealth.org). Modern medicine recognizes that appendicitis is primarily a disease of the Western World.31 They attribute this to the (allegedly) greater amount of fiber in the diet of the Third World. However, the fiber theory has never been substantiated, as evidenced by this quote from www.KidsHealth.org: There are no medically proven ways to prevent appendicitis. Although appendicitis is rare in countries where people eat a high-fiber diet, experts have not yet shown that a high-fiber diet definitely prevents appendicitis.Many residents of the developing world, not wanting to appear "backward", feel obliged to adopt western toilets. This trend is causing health problems that were previously unknown among squatting populations. Appendicitis is one example, as reported by webhealthcentre.com, a health care portal based in India (retrieved in 2001): The Indian type of toilet is more conducive to complete evacuation than the Western toilet. With the western style closets becoming popular in India, there is a risk of increased incidence of appendicitis.Unfortunately, western doctors have never made the connection between toilet posture and appendicitis. Their understanding of this disease has advanced little in the century since Dr. Frederick Treves performed his famous appendectomy (mentioned above) on the Prince of Wales. Ironically, Sir Frederick (knighted for saving the king's life) lost his own daughter to appendicitis.27 Despite being highly skilled at surgery, he had no idea what causes the disease, or how to prevent it.Now his successors have a chance to redeem their profession. By informing their patients (and their children) about the health hazards of the modern toilet, they can prevent a great deal of needless suffering. top of page |
... a chronic and serious inflammatory disease of the gastrointestinal tract that affects more than 500,000 Americans. People with Crohn's disease may experience a number of symptoms including diarrhea, abdominal cramps and pain, fever, rectal bleeding, loss of appetite, and weight loss....The cause of Crohn's disease has not yet been discovered.Inflammatory bowel disease (IBD) includes Crohn's Disease, ulcerative colitis and irritable bowel syndrome. IBD affects approximately 2 million Americans and can have devastating consequences. 20 to 40% of ulcerative colitis patients eventually require surgery for removal of the colon, according to the University of Maryland Medicine website. Up to 70% of patients with Crohn's disease require surgery at some point in their disease course to remove parts of the intestine.IBD is confined to countries of the Western World, according to a study published in The Lancet.21 A 1997 article reported that "The last half of this century has seen a rising incidence of inflammatory bowel disease in developed countries," but notes "... the apparent absence of IBD in developing countries." [italics added] For many years, researchers assumed that a different diet was protecting the developing world from IBD. "What else could it be?" They did not realize that these cultures have no uniform diet. For example, the Masai cattle-herders of central Africa are almost exclusively carnivorous. The Hindus of India are vegetarian. Other groups subsist on fish, or even on insects. On testing their hypothesis, doctors were forced to conclude that "No special diet has been proven effective for preventing or treating this disease." (from the University of Chicago Hospitals website.) Currently another theory has become popular among epidemiologists. They believe that fecal contamination of food and water in the developing world "naturally innoculates" children against inflammatory bowel disease. In other words, the Western World is too antiseptic to allow the immune system to produce the necessary antibodies. This theory reflects a common misconception about the "superior hygiene" of the developed world. Westernized countries are proud of their high standards of cleanliness, but they are unaware that their internal cleanliness compares poorly with the rest of the world. Colon hygiene depends on the effectiveness of daily elimination. Human beings were designed to perform their bodily functions in the squatting position. In order to be squeezed empty, the colon needs to be compressed by the thighs. Furthermore, the puborectalis muscle needs to be relaxed and the ileocecal valve from the small intestine needs to be closed. By ignoring these requirements, the sitting toilet makes it impossible to empty the colon completely. Incomplete evacuation causes wastes to stagnate in the lower regions of the colon. In these areas, virulent bacteria can establish colonies, inflaming the surrounding tissues. Depending on where in the colon it occurs, and which strain of bacteria is involved, this inflammation is called by different names. Appendicitis, diverticulitis, ulcerative colitis, and Crohn's Disease can all be considered as various forms of inflammatory bowel disease. (Ileitis will be discussed below.) Therefore, what protects the developing world is not "squalid conditions" but just the opposite: the natural cleanliness that comes from evacuating as nature intended. The relevance of toilet posture is also confirmed by the historical evidence. Inflammatory bowel disease and irritable bowel syndrome emerged in the West toward the end of the 19th century, as the use of sitting toilets became more and more common.22,28 This explanation is supported by a recent article in HealthScout News entitled "E. Coli Linked to Inflammatory Bowel Disease" (February 5, 2002): An intestinal infection caused by strains of a common bacterium may be linked to the development of inflammatory bowel disease, a new study says. French researchers report that a heightened immune interaction between Escherichia coli and the cells lining the intestine may result in the symptoms experienced by people with inflammatory bowel disease (IBD). They suggest their work indicates antibiotics might be a useful tool when treating IBD.Another form of Crohn's Disease is "ileitis" or inflammation of the small intestine. It results from fecal matter being forced backwards into the small intestine during evacuation. The ileocecal (IC) valve is designed to prevent this toxic "backflow" – but only in the squatting position. The IC valve needs to be supported by the right thigh in order to withstand the pressure built up during elimination. A more detailed explanation of this process can be found in two other sections: Contamination of the Small Intestine and Appendicitis. The anatomy and demographics of inflammatory bowel disease imply that squatting would be useful for prevention. Anecdotal evidence suggests its potential for use in treatment as well. Mr. Wallace Bowles, an Australian researcher, has extensively reviewed the medical literature and has surveyed converts to the natural squatting position: I have received reports regarding several people, aged between 5 and 45 years, diagnosed with Crohn’s Disease. Inflammatory bowel conditions are shown to react most positively when the cumulative injury of seated elimination is relieved by squatting. People with IBD who have changed to the squat posture for bowel movements report significant improvement within a few weeks and, in time, have lost all symptoms of this horrendous condition.More research is clearly needed, but it can be easily and non-invasively done by any gastroenterologist or any patient with colitis or Crohn's Disease. Each successful outcome will not only relieve the patient's own suffering, but will also help to validate a promising strategy to prevent inflammatory bowel disease. Note: The book Triumph Over Disease By Fasting And Natural Diet, by Jack Goldstein, recounts a remarkable self-cure of ulcerative colitis after the failure of conventional treatment. top of page |
The sitting toilet obstructs the flow, because it ignores four basic requirements:
For safety, nature has deliberately created obstacles to evacuation that can only be removed by squatting. In any other position, the colon defaults to "continence mode." This is why the conventional sitting position deprives the colon of support from the thighs and leaves the rectum choked by the puborectalis muscle. These obstacles make elimination difficult and incomplete – like trying to drive a car without releasing the parking brake. Chronically incomplete evacuation, combined with the constant extraction of water, causes wastes to adhere to the colon wall. The passageway becomes increasingly constricted and the cells start to suffocate. Prolonged exposure to toxins will often trigger malignant mutations. This explanation would suggest that colon cancer is related to constipation. According to a 1998 report in the journal, Epidemiology,3 "People who frequently felt constipated were more than four times as likely to develop colon cancer as those who did not complain of constipation." The study also found that using commercial laxatives frequently was associated with "substantially increased risk of colon cancer." Colorectal cancer, however, is not uniformly common throughout the world. There is a large geographic difference in the global distribution of colorectal cancer. Colorectal cancer is mainly a disease of developed countries with a Western culture. In fact, the developed world accounts for over 63% of all cases. The incidence rate varies up to 10-fold between countries with the highest rates and those with the lowest rates.For decades, researchers have been trying to explain the absence of colon cancer in the developing world. Some have speculated that perhaps E. coli bacteria in the water and food somehow stunts the growth of cancer cells in the intestine.This theory reflects the common belief that our society is "clean" while the developing world is "dirty." In terms of colon hygiene, exactly the opposite is the case. What protects the developing world from bowel disease is the natural cleanliness that comes from evacuating as nature intended. By contrast, our contrived toilet posture leads to fecal stagnation – the primary cause of colon cancer and inflammatory bowel disease.  Lacking this knowledge, researchers have focused on dietary factors. They have repeatedly tried to prove that a high-fiber diet prevents colon cancer. This theory dates from the early 1970's when Dr. Denis Burkitt (1911-1993), a British missionary doctor (pictured here), reported a dramatic difference between colon cancer rates in America and Africa. According to his article in the Journal of the Royal Society of Medicine, colon cancer is nearly 15 times as common in black Americans as in Africans.40 Lacking this knowledge, researchers have focused on dietary factors. They have repeatedly tried to prove that a high-fiber diet prevents colon cancer. This theory dates from the early 1970's when Dr. Denis Burkitt (1911-1993), a British missionary doctor (pictured here), reported a dramatic difference between colon cancer rates in America and Africa. According to his article in the Journal of the Royal Society of Medicine, colon cancer is nearly 15 times as common in black Americans as in Africans.40The above article appeared on October 13, 2000. Five years later, medical researchers – at their wits' end – were still testing the same discredited theory. On December 14, 2005, The Boston Globe reported on the latest attempt by the Harvard School of Public Health: Eating a lot of fiber-rich vegetables, fruits, and whole grains does not appear to reduce a person's chances of getting colorectal cancer, researchers found in the largest study yet to test the popular and longstanding idea about preventing the third most common cancer...."It became an urban myth," said Dr. David Ryan, medical director of the gastrointestinal cancer center at Massachusetts General Hospital. ''It takes a lot of time to deconstruct those.".... [Full Article] Western researchers ignored this hypothesis, partly because toilet posture was considered a taboo subject. They also probably believed that the western world could never revert to squatting, even if sitting toilets were proven to be harmful. So, they simply hoped that modifying the diet would be enough.Now that the fiber theory has clearly failed, they will have to reconsider Dr. Burkitt's alternate explanation. They may be surprised by the public's openness to a simple change that could save many lives. top of page |
Constipation has been shown to increase the risk of colon cancer3 and has been implicated in diverticulosis and appendicitis. "Cumulative lifetime use of commercial laxatives was also associated with increased risk of colon cancer."3 Squatting prevents constipation in four ways:
The sphincter muscle, commonly regarded as the outlet valve, is actually not capable of preventing incontinence. It involves voluntary effort and is only for short-term emergencies. Maintaining continence requires the continuous grip of the puborectalis muscle. This grip is not released in the sitting position, so it must be forced open by straining. Straining repeatedly over a number of years can lead to hemorrhoids, which can therefore be classified as a repetitive strain injury. Doctors have long recognized the connection between sitting toilets and constipation. For example, F.A. Hornibrook in The Culture of the Abdomen,published in 1933: Man's natural attitude during [elimination] is a squatting one, such as may be observed amongst field workers or natives. Fashion, in the guise of the ordinary water closet, forbids the emptying of the lower bowel in the way Nature intended. Now in this act of [elimination] great strains are imposed on all the internal organs….It is no overstatement to say that the adoption of the squatting attitude would in itself help in no small measure to remedy the greatest physical vice of the white race, the constipation that has become a contentment.5uThese sentiments are echoed in Our Common Ailment, written by H. Aaron and published in 1938: When the thighs are pressed against the abdominal muscles in this position, the pressure within the abdomen is greatly increased, so that the rectum is more completely emptied. Our toilets are not constructed according to physiological requirements. Toilet designers can do a good deal for people if they will study a little physiology and construct seats intended for proper [elimination].6top of page |
Thirty subjects participated in the study – 21 male, 9 female – ranging in age from 11 to 75 years. Each patient received a barium enema so the internal mechanics of evacuation could be recorded on an X-Ray image. Each patient was studied in both the squatting and the sitting positions. Using these images, Dr. Rad measured the angle where the end of the rectum joins the anal canal. At this junction point, the puborectalis muscle creates a kink to prevent incontinence. Dr. Rad found that when the subjects used sitting toilets the average angle of this bend was 92 degrees, forcing the subjects to strain. When they used squat toilets, the angle opened to an average of 132 degrees. At times it reached 180 degrees, making the pathway perfectly straight. Using squat toilets, all the subjects reported "complete" evacuation. "Puborectalis relaxation occurred easily and straightening of the rectum and anal canal facilitated evacuation. The anal canal became wide open and no folding was noticed in the terminal rectum." In the sitting position, "a remarkable folding was created in the terminal rectum predisposing it to rectocele formation, and puborectalis relaxation was incomplete." All the subjects reported that elimination felt "incomplete" in the sitting position. Dr. Rad also measured the distance from the pelvic floor to the perineum. In the sitting position he found that the pelvic floor was pushed downwards to a significant degree. (A detailed discussion of the connection between sitting toilets and pelvic organ prolapse – including rectoceles – can be found in the gynecological disorders section.) Dr. Rad concluded that the use of the squat toilet "is a more comfortable and efficient method of bowel evacuation" than the sitting toilet.  Different types of squat toilets |
The ileocecal (IC) valve, between the small intestine and the colon, is designed to prevent the backflow of wastes. If it leaks, E.coli bacteria can enter the small intestine and get absorbed into the bloodstream. This puts a strain on the liver which has to remove these toxins. The invasion of fecal bacteria (called "colo-ileal reflux") can also cause inflammation of the small intestine. This condition is called "ileitis" and is a form of Inflammatory Bowel Disease. According to Dr. Welles, My discovery of a dysfunctional ileocecal valve in approximately 80% of my patients is also confirmed by modern medicine. The ICV is so commonly found to be dysfunctional in surgeries of the bowel and in barium enema studies that it is believed to be inherently faulty in its design.2Drawing on the research of F.A. Hornibrook, Dr. Welles suspected that the faulty design responsible for this problem was not nature's but man's. Hornibrook states that the design of the Western toilet defies the laws of nature by encouraging the user to bear down without the natural support given the abdominal walls by the thighs when one is in the squatting posture.2Then, he used muscle-testing to verify his hypothesis. When individuals sat in the position encouraged by the western toilet and bore down so as to eliminate fecal matter, the muscles weakened immediately and the ileocecal valve was blown out....The ICV is critical to proper intestinal plumbing, and its dysfunction is the root cause of many of the diseases of modern civilization.... 2In his article, Dr. Welles also discusses other ailments caused by the sitting toilet – including colon cancer, hemorrhoids, hernias and pelvic organ prolapse. He concludes with some strong words of advice: Cast aside your preconceived ideas as to what is normal and use your rational mind to act on what has been stated above. At any given time in history it is possible to look back and find great faults with the habits of previous civilizations. I believe that future generations will one day look back at our aberrant habit of using the modern toilet – and cringe. 2top of page |
 Diverticulosis is a type of hernia caused by years of chronic straining. The outer layer of the colon ruptures, allowing the inner lining (the "mucosa") to bulge out in pouches or sacs. It is similar to an inner tube that bulges out through weak spots in a worn-out tire. Diverticulosis is a type of hernia caused by years of chronic straining. The outer layer of the colon ruptures, allowing the inner lining (the "mucosa") to bulge out in pouches or sacs. It is similar to an inner tube that bulges out through weak spots in a worn-out tire.Diverticulosis typically occurs in the sigmoid colon, in the lower left section of the abdomen. According to the National Digestive Diseases Information Clearinghouse: About half of all Americans age 60 to 80, and almost everyone over age 80, have diverticulosis. When the pouches become infected or inflamed, the condition is called diverticulitis. This happens in 10 to 25% of people with diverticulosis...... Diverticulitis can lead to complications such as infections, perforations or tears, blockages, or bleeding. These complications always require treatment [surgery] to prevent them from progressing and causing serious illness.1These statistics might seem to imply that diverticulosis is an inevitable part of growing old. Dr. Berko Sikirov, the Israeli physician who conducted successful clinical research on the use of squatting to treat hemorrhoids, disagrees: Colonic diverticulosis develops as a result of excessive straining at defecation due to habitual bowel emptying in a sitting posture, which is typical of Western man. The magnitude of straining during habitual bowel emptying in a sitting posture is at least three-fold more than in a squatting posture and upon urge. The latter defecation posture is typical of latrine pit users in underdeveloped nations.The bowels of Western man are subjected to lifelong excessive pressures which result in protrusions of mucosa through the bowel wall at points of least resistance. This hypothesis is consistent with recent findings of elastosis of the bowel wall muscles, the distribution of diverticula along the colon, as well as with epidemiological data on the emergence of diverticulosis coli as a medical problem and its geographic prevalence.9The geographic prevalence mentioned by Dr. Sikirov is confirmed by medicinenet.com, a well-respected medical website: Diverticular disease is common in the Western world but is extremely rare in areas such as Asia and Africa.Mainstream medicine has never considered the relevance of evacuation posture to diverticulosis. They attribute its high prevalence in our society to "insufficient dietary fiber." But they offer no evidence to support their theory. (The same theory was used for decades to explain colon cancer until it was disproved by several recent studies.)An excerpt from The Mayo Clinic on Digestive Health illustrates a common fallacy used to promote the theory: Diverticular disease emerged after the introduction of steel rolling mills, which greatly reduced the fiber content of flour and other grains. The disease was first observed in the United States in the early 1900's around the time processed foods became a mainstay of the American diet ...23The Mayo Clinic is correct to blame a technological innovation – but which one?The same Industrial Revolution that produced the steel rolling mill also made the porcelain throne a fixture throughout the western world.22Dr. Denis Burkitt, the British surgeon who popularized the fiber theory, also strongly advocated the use of squat toilets to prevent diverticulosis and hiatus hernias.41 His only mistake was to assume that diet was the crucial factor and squatting was secondary, instead of the other way around. The claim that dietary fiber protects against diverticulosis was finally tested in a recent study involving 2,104 participants, 30–80 years old. They underwent outpatient colonoscopies from 1998 to 2010 and were interviewed regarding diet and physical activity. The study, published in the February, 2012 issue of Gastroenterology, found that "A high-fiber diet and increased frequency of bowel movements are associated with greater, rather than lower, prevalence of diverticulosis. Hypotheses regarding risk factors for asymptomatic diverticulosis should be reconsidered." In a media interview, the lead author, Anne F. Peery, MD put it more bluntly:"Our study makes it clear that we don't really understand why diverticula form." The journal article also discusses the impact of this disease on health care costs:"The complications of diverticulosis cause considerable morbidity in the United States; health care expenditures for this disorder are estimated to be $2.5 billion per year." To solve their "mystery," the researchers need to examine the biomechanics of evacuation. They will find that a western toilet strains the sigmoid colon in three ways:
As we bear down without proper support, it increases the degree of kinking at this junction, and limits the amount of elimination to whatever is below the kink. 2Straining is therefore counterproductive – but unavoidable – as long as we persist in using an unnatural toilet posture. The self-inflicted injury called "diverticulosis" is the inevitable result. |
In 1990 he published an article entitled "Cardio-vascular events at defecation: are they unavoidable?" He begins by describing the problem: Probably every physician practicing emergency medicine has encountered tragic cases of sudden death in the lavatory. Patients with acute coronary events are especially vulnerable to excessive straining which accompanies defecation. Therefore, it is a routine practice in coronary care units to administer laxatives or stool softeners, hopefully to reduce straining ...10The article goes on to explain how straining on the toilet can be avoided by adopting the natural squatting position. In the following summary, Dr. Sikirov uses the term "Valsalva Maneuver," which means pushing down with the diaphragm while holding one's breath. According to the American Heritage Dictionary, this maneuver "increases pressure within the thoracic cavity and thereby impedes venous return of blood to the heart." Another term used below is "syncope" which means "fainting." Cardio-vascular events at defecation are to a considerable degree the consequence of an unnatural (for a human being) seated defecation posture on a common toilet bowl or bed pan. Excessive straining, expressed in intensively repeated Valsalva Maneuvers, is needed for emptying the bowels in the sitting position. The Valsalva Maneuver adversely affecting the cardio-vascular system is the causative factor of defecation syncope and death.The cardio-vascular system of a healthy man withstands the intensive and repeated straining at defecation, while the compromised cardio-vascular system may fail, resulting in syncope or even death. The squatting defecation posture is associated with reduced amounts of straining and may prevent many of these tragic cases.10Besides straining the heart, the Valsalva Maneuver also leads to pelvic organ prolapse, discussed in the Gynecological Disorders, Pregnancy, and Prostate Disorders sections.top of page |
The common explanation for their absence in the developing world is "a high fiber diet." An Internet search on "incidence of hemorrhoids" turns up many instances of the following statement, carefully worded to suggest a causal connection: "Populations in which fiber intake is high have a very low incidence of hemorrhoids." The medical establishment accepted the fiber theory without proof because they had no other explanation for the dramatically lower incidence of hemorrhoids in the developing world. They ignored the fact that these populations follow a wide variety of diets. The Masai cattle-herders of central Africa are almost exclusively carnivorous. The Hindus of India are vegetarian. Other groups subsist on fish, or even on insects. Researchers have also been unaware of another, more relevant factor which would explain the data: the use of squat toilets. This factor has three advantages over the fiber theory:
Twenty male and female patients who had hemorrhoids of varying degrees of severity participated in the study. They had all used conventional treatments with little or no success. Two of the patients had been treated with ligation (tying off the hemorrhoid at its base with a rubber band.) The patients underwent a proctoscopy at the beginning of the trial. Then they were told to change their toilet habits in two ways: to wait until the urge to evacuate was strong (to avoid straining) and to use the natural squatting position for elimination. The proctoscopy was repeated after one year. Of the 20 patients, 18 reported within a few days to a few months a significant reduction or complete absence of symptoms. Lack of improvement in the two other patients, who had previously had ligation for hemorrhoids, "may be ascribed to fibrous tissue development in the submucosa as a consequence of the ligation."7 Follow-up examinations, 12 and 30 months later, on the 18 other patients (90% of the subjects in the study), revealed no recurrence of the symptoms. This chart shows the results obtained by all 20 patients. A detailed account of Dr. Sikirov's research can be found in his U.S. Patent #4,819,277. Dr. Sikirov's conclusion is that hemorrhoids result from continual aggravation and injury due to excessive straining in the sitting position. Straining is necessary to overcome the constriction in the rectum designed to maintain continence. When this ongoing insult to the body is removed by returning to the squatting position, the natural healing process can occur without hindrance. The importance of squatting is not unknown to gastroenterologists and proctologists. Dr. Michael I. Freilich, a retired colorectal surgeon from Marina del Rey, California, recently commented, Back in 1979, when former President Carter had a hemorrhoid problem, Time Magazine called and asked me to explain the cause of hemorrhoids. In the magazine, I was quoted as saying, "Man was not meant to sit on a toilet, but to squat in a field."Even the standard textbook, Bockus Gastroenterology, contains the statement, "The ideal posture for [evacuation] is the squatting position, with the thighs flexed upon the abdomen. In this way the capacity of the abdominal cavity is greatly diminished and intra-abdominal pressure is increased, thus encouraging expulsion ..."11Unfortunately, most proctologists pretend to be unaware of the therapeutic value of squatting. Surgery and ligation are lucrative procedures. Not wanting their income to suffer, they cause their patients to suffer instead. top of page |
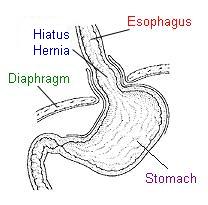 A hiatus hernia (also called "hiatal hernia") occurs when the upper part of the stomach bulges into the chest cavity through a tear or weakness in the diaphragm. It is often associated with GERD (gastroesophageal reflux disease) in which stomach acid leaks into the esophagus. GERD causes chronic heartburn and increases the risk of esophageal cancer. A hiatus hernia (also called "hiatal hernia") occurs when the upper part of the stomach bulges into the chest cavity through a tear or weakness in the diaphragm. It is often associated with GERD (gastroesophageal reflux disease) in which stomach acid leaks into the esophagus. GERD causes chronic heartburn and increases the risk of esophageal cancer.Hiatus hernia has its maximum prevalence in economically developed communities in North America and Western Europe. Very large series of upper gastrointestinal tract radiological examinations indicate that this defect can be demonstrated in over 20% of North American adults [of all races].In contrast, the disease is rare in situations typified by rural African communities. In a careful prospective radiological study of the upper gastrointestinal tract in Nigerians, hiatus hernia was detected in only four of 1030. In Kenya, only one case was found in over 1000 barium meal examinations and in Tanzania, one in over 700 barium studies.41In 1999, gastroenterologist Dr. Stephen Sontag expanded still further the indictment of the western toilet. The following excerpt summarizes his paper, "Defining GERD," published in the Yale Journal of Biology and Medicine: 42 The antireflux barrier in children and adults is gradually weakened over time as a result of chronic straining to defecate and straining in an unphysiologic position, both of which stem from our modern day habits of eating a low-fiber diet and living on the high-seated toilet. We suggest that the chronic traumatic hiatal hernia isDr. Sontag's detailed explanation, contained in his twelve-page article, can be found at the journal's website.To summarize, the diaphragm was not designed to be the "workhorse" for evacuation. Like all primates, humans were designed to squat for bodily functions. Squatting pushes the colon against the thighs by the force of gravity and effortlessly creates the required pressure for expulsion. The daily abuse of the diaphragm caused by the western toilet is the reason for the high incidence of hiatus hernias and GERD in our society. top of page |
Although he had no formal medical training, his intense curiosity led him to immerse himself in the study of human anatomy, in order to understand why squatting for bodily functions was so much more effective. He also suspected that the habitual use of sitting toilets might be responsible for some common ailments found only in westernized countries. As a man in his fifties, Mr. Bowles was naturally curious about a possible connection to prostate problems. He was intrigued by evidence such as the following: from USA Today, January 5, 2000:In his review of the medical literature, Mr. Bowles encountered the usual explanation for the low incidence of prostate cancer in the developing world: a diet low in fat and high in fiber. He was skeptical of this theory, and a recent major study has confirmed his doubts: (American Society of Clinical Oncology - August 30, 2002) – A low-fat, high-fiber diet heavy in fruits and vegetables has no impact on PSA levels in men over a four-year period, and does not affect the incidence of prostate cancer, according to a study by researchers at Memorial Sloan-Kettering Cancer Center, the National Cancer Institute, and seven other centers.Mr. Bowles took an entirely different approach to the problem. He suspected that the prostate's strange behavior was caused by a breakdown in the body's system of communication and control. The prostate and bladder are controlled by the pudendal nerve, which emerges from the sacrum, near the base of the spine, and runs along the perineum. Damage to this nerve can weaken the brain signals to and from the prostate and render the gland dysfunctional. In women, the pudendal nerve is commonly injured during childbirth, leading to temporary or permanent bladder incontinence. Pelvic nerve injury often results from instrumental deliveries (forceps, vacuum extractors, etc.) and from straining to overcome the unnatural western delivery posture. (More details in the Pregnancy and Childbirth section.) But childbirth is not the only way the pudendal nerve is damaged. It happens to women who have never had children, as well as to men. Mr. Bowles theorized that the same stretching of the pelvic floor caused by giving birth in the recumbent position could also result from evacuating in the sitting position. Bowel evacuation is not as stressful as childbirth, but is repeated on a daily basis. The pelvic floor is a hammock of muscles which supports the bladder, the intestines and (in women) the uterus. The pudendal nerve travels from the spinal cord through the pelvic floor to the bladder and prostate. On a conventional toilet, the pelvic floor is unsupported and is forcefully pushed downwards during evacuation. The practice of holding one's breath and pushing with the diaphragm is considered "normal" in western societies. But no other animal uses this "Valsalva Maneuver." Like all primates, man was designed to use the squatting position, which empties the colon without putting any pressure on the pelvic floor. Instead of pushing downwards with the diaphragm, squatting pushes upwards with the thighs. The weight of the torso compresses the colon, so no straining is required. Squatting also relaxes the puborectalis muscle to straighten the rectum. This is the method used by over two-thirds of humanity. How does seated evacuation damage the pudendal nerve? The nerve passes through the pelvic floor and has to stretch each time the Valsalva Maneuver is used. Nerves are not elastic and cannot be stretched very far without being damaged. A 12% stretch destroys a nerve. 16 Over the years, the pelvic hammock sags lower and lower, from being pushed downwards several times each day. The pudendal nerve is eventually stretched beyond its capacity. It loses the ability to transmit brain signals and supply electrical energy to the pelvic area. Every gland in the body requires constant feedback from the brain to maintain normal functioning. Damage to the pudendal nerve disconnects the prostate from the body's governing intelligence. The prostate "loses its mind" – as millions of men discover each year, to their dismay. Prostate disease affects 75% of the male population over the age of 50.39 It can take three different forms:
Damage to the pudendal nerve occurs gradually and cumulatively and can take many years to manifest. This is one reason why the cause has escaped detection. Another reason is cultural insularity. Sitting toilets were considered normal and natural and so, above suspicion. To test his theory, Mr. Bowles designed and manufactured a squatting device, and encouraged thousands of his fellow Australians to adopt the natural posture for evacuation. Here is his summary of the results: An ongoing informal study indicates that, providing prostate enlargement has not progressed too far, symptoms gradually reverse when men abandon seated bowel movements and squat instead. The study indicates that improvement usually occurs within three months and, within about six months of making this posture change, most men (including men in their seventies) regain normal prostate function. 14Mr. Bowles concluded that the damaged nerves will grow back over time if the source of injury is removed. Many respondents also reported significant reductions in their PSA levels (prostate specific antigen) after switching to squatting. Wallace Bowles did not invent the concept of "pelvic floor nerve stretch injury." He simply realized that this self-inflicted injury has been institutionalized by the universal habit of sitting for evacuation. He therefore concluded that the porcelain throne is the most likely culprit in the mysterious epidemic of pelvic disorders (male and female) that plagues the Western World.This "eureka!" of a retired aircraft accident investigator may someday be recognized as one of the most important breakthroughs in the history of medicine. top of page |
Bladder Incontinence
In the larger cities of Asia, many residents have abandoned their traditional customs, believing that the West is more progressive and somehow "superior." By adopting western toilets, they have unwittingly introduced new diseases into their society. A recent article in the Malaysian newspaper The Star (March 30, 2003) discusses one such ailment:To squat or not to squat? That is the question. Actually, your toileting technique may have an effect on urinary incontinence. There is a lot of evidence to show that the Asian technique of using the toilet goes a long way to maintaining better pelvic health than the Western technique, says professor Ajay Rane, James Cook University of Medicine (Australia) consultant urogynecologist and pelvic reconstructive surgeon.According to Rane, a study done in Hong Kong showed that city-dwelling women had more urinary incontinence and bowel problems than country dwelling women. "The basic differences in these women were not their body weight, or how many children they had, but their toileting habits," he says.In general, women in urban areas use the "sit" method while the rural women use "squat" toilets. "Basically, we believe that the study suggests squatting causes the angle of the pelvis to relax much better and give better pressure. When you are sitting, you do not have the right relaxation of the muscles and the angle of the pelvis," he says. "I strongly believe that the squatting technique has tremendous beneficial effects on the pelvis."Dr. Rane's view is shared by Dr. Stuart Stanton, Chairman of the Continence Foundation and Consultant Urogynecologist at St. George's Hospital, London: "Squat" toilets are an excellent way for women to exercise their perineum and pelvic floor muscles and control their urinary stream from the age of 2½-3 years onwards. Reports from the developing world suggest that urinary incontinence is much less in women who squat.Here is a brief explanation of why sitting toilets increase the risk of incontinence: The pelvic floor is a hammock of muscles that supports the intestines, the bladder and the uterus. Western toilets force the user to strain when evacuating, repeatedly subjecting the pelvic floor to unnatural stress. The downward pressure stretches and weakens the pudendal nerve, responsible for bladder control. To maintain continence, the brain needs to constantly monitor the pressure within the bladder and issue commands to the urethral sphincter muscle. Both functions are impaired when the pudendal nerve is weakened by the descent of the pelvic floor. The following statistics from FocusOnUrology.com show how frequently this occurs:
An unnatural maneuver repeated so many times inevitably causes a "repetitive stress injury." The pudendal nerve is the main casualty of this unintentional abuse, which renders incontinent over 50% of elderly Americans (statistics above.) Other westernized countries face a similar problem. Researchers at Adelaide University in Australia recently reported that incontinence and other pelvic floor disorders are much more prevalent than previously believed. The article is entitled "The Descent of Women – a Silent Epidemic" (23 November 2000): Adelaide University researchers, in the first comprehensive study of its kind in the world, have found a remarkably high prevalence of pelvic floor disorders in the general population.... Most of these complaints were still common among women who had never had a vaginal birth.... "The survey highlights the high prevalence and major social impact of pelvic floor prolapse and incontinence in our society," said Professor MacLennan. "It is a silent epidemic, as those with the problem are often embarrassed to talk about it," he said.Until recently, the cause of this epidemic has been a mystery (Professor MacLennan, quoted above, believes that it is unavoidable, as long as women continue to give birth.) But research by Mr. Wallace Bowles on the relevance of the squatting posture has brought a new understanding of how to prevent (and, in many cases, correct) these disorders: Most people with urinary incontinence experience a noticeable improvement within several weeks of commencing to squat for defecation with complete correction within about 3 months.17Anecdotally, a number of women who squat, habitually, for bowel movements and who have experienced pelvic floor trauma and incontinence after the birth of their baby, have regained their continence within about six weeks when they continue to adopt the squat posture for bowel evacuation.13Even children are susceptible to pelvic floor nerve stretch injury. An article entitled "My Child, My Teacher" was published in the Spring, 1998, issue of New Vegetarian and Natural Health Magazine.15 Focusing on the benefits of squatting for children, the article contains numerous reports of bedwetting corrected by this simple change of habit.top of page |
Pregnancy and Childbirth Issues
Childbirth educators always advise pregnant women to avoid the "Valsalva Maneuver," which means holding one's breath while straining. It puts great pressure on the uterus and the pelvic floor.Unfortunately, this maneuver is impossible to avoid when using a conventional toilet. This is why expectant mothers find daily elimination such an uncomfortable and frustrating experience. Constipation during pregnancy is considered "normal" because most doctors are unaware of the abnormal design of the modern toilet. Besides improving elimination, squatting also helps in other ways during pregnancy:
A study published in 1969 in the Journal of Obstetrics and Gynaecology of the British Commonwealth found that squatting increases the available area in the birth canal by 20 to 30%.25 The sitting toilet has made women incapable of prolonged squatting, which would promote a quicker and more comfortable labor and delivery. It would also reduce the need for medical interventions such as forceps, vacuum extractors, epidurals and episiotomies. The most drastic form of medical intervention is the cesarean section. 32% of US births in 2007 were by C-section.37 This alarming statistic indicates that women are losing the ability to give birth naturally. The modern toilet has alienated women from the birthing posture they were designed to use. The conventional delivery positions – recumbent and semi-sitting – close the birth canal by 20 to 30%.25 The baby is used as a "wedge" to force the birth canal open. Obstetricians, unaware of what is causing the obstruction, resort to drugs and elaborate appliances to "extract" the fetus. Their crude and forceful procedures increase the risk of injury to mother and baby. Almost all hospital delivery rooms prohibit the use of the squatting position, so women are forced to use the Valsalva Maneuver. They hold their breath and push with all their might – oblivious to the fact that the birth canal is partially closed. This maneuver puts enormous strain on the pelvic floor. A common result is damage to the pudendal nerve, which connects the pelvis to the spinal cord. Nerve damage can lead to bladder incontinence and hormonal imbalance, due to the breakdown in communication between the brain and the pelvis. Post-partum depression is one symptom of hormonal imbalance. Giving birth in the squatting position does not require the Valsalva Maneuver. Besides fully opening the birth canal, the posture naturally compresses the abdominal cavity to push the baby along, without great exertion or holding of breath. The full squatting posture also minimizes the risk of pelvic hernias, often caused by straining during delivery. The bladder, the uterus, or the intestines can be dislodged from their proper place and pushed into the vagina. These hernias are extremely common in the western world. But in the developing world, where squatting is used, women are "relatively unaffected by pelvic floor problems."36 Human beings should be able to give birth as easily as any other animal. This is the case for over two-thirds of the world's women, since they use the same posture they have used all their lives for bodily functions.By rediscovering how the body was designed to function, women can greatly reduce the stress of pregnancy and childbirth. Having a baby will never be effortless, but it can become a much safer, easier and more joyful experience. top of page |

Gynecological Disorders
Each year more than 600,000 hysterectomies are performed in the United States. About one-third of American women undergo this operation by the age of 60.It is performed to deal with a number of different diseases, including uterine fibroids, endometriosis, uterine prolapse and cancer. More information about hysterectomies can be found at the National Women’s Health Information Center website. The website states that "no one knows the cause" of these diseases. But the fact that one out of every three women has her uterus removed indicates that something in our culture is fundamentally wrong. Before the 19th century, hysterectomies were so rare that "most doctors were of the opinion that it was unlikely that one could survive a hysterectomy." 32 The sharp increase in uterine disorders toward the end of the 19th century coincided with a similar rise in prostate disorders,33 leading to the suspicion that the two trends were somehow connected. The connection became clearer as doctors learned more about another common pelvic ailment: bladder incontinence. They found that it typically results from damage to the pudendal nerve, which connects the pelvis to the spinal cord. This damage was traced to a "stretch injury" – caused by the progressive descent of the pelvic floor. Furthermore, they recognized that the porcelain throne is an "ergonomic nightmare" because it forces one to use the Valsalva Maneuver (holding one's breath and pushing down with the diaphragm.) No other animal uses this maneuver. The pelvic floor was not designed to handle this type of stress on a daily basis. Like all primates, man was designed to use the squatting position, which empties the colon without putting any pressure on the pelvic floor. Instead of pushing downwards with the lungs, one pushes upwards with the thighs, in the following way: The right thigh pushes the cecum's contents upward into the ascending colon. The left thigh squeezes and lifts the sigmoid colon, and opens the kink where it joins the rectum. Squatting also relaxes the puborectalis muscle to open the outlet valve. A conventional toilet defeats the purpose of this ingenious design. Trying to evacuate while sitting is like trying to drive a car without releasing the parking brake. In frustration, one pushes down forcefully – depressing the pelvic floor many times each day. Over the years, the pelvic floor gradually descends more and more, and stretches the pudendal nerve beyond its capacity. Cut off from the source of energy and intelligence, the pelvic organs become dysfunctional and prone to disease. Cancer, endometriosis and uterine fibroids can be viewed as different forms of "dementia" on the cellular level. Endometriosis provides a good illustration of how cells behave when they lose contact with the brain. In this disease, the cells lining the uterus wander off and attach themselves to other organs – much like an Alzheimer's patient who has forgotten where she lives. "Endometriosis is a painful, chronic disease that affects 5.5 million women and girls in the USA and Canada, and millions more worldwide." (Endometriosis Association) It is the second leading reason for hysterectomies. Repeated use of the Valsalva Maneuver will often force the uterus, the bladder, the rectum or the small intestine into this gap. These hernias are called, respectively, uterine prolapse, cystocele, rectocele (pronounced REK-tuh-seel), and enterocele (pronounced EN-tuh-ruh-seel). The term "pelvic organ prolapse" covers all of them. Rhonda Kotarinos, MS, PT, is a renowned physical therapist who has trained physicians at Stanford Medical School in techniques for treating pelvic floor problems. In a recent lecture to members of the Interstitial Cystitis Network, she stated that long-term Valsalva voiding leads to pelvic organ prolapse.38 The risk of prolapse is even greater during childbirth, when the Valsalva Maneuver is employed with maximum force. Here again, the modern toilet is to blame, because it has alienated women from the birthing posture they were designed to use. As explained in the Pregnancy and Childbirth section, squatting fully opens the birth canal and virtually eliminates the need for the Valsalva Maneuver. This is why women in the developing world are "relatively unaffected by pelvic floor problems"36 while the United States spends more than $10 billion each year on pelvic reconstructive surgery and $26 billion to treat urinary incontinence.36 The high rate of C-Sections is another consequence of using the wrong posture for delivery. Natural (vaginal) childbirth is feared because it is performed in an unnatural and dangerous way. 32% of US births in 2007 were by C-section.37 But their theory ignores the fact that the pelvic floor has performed quite adequately throughout human history, with only rare exceptions. It is only recently, in modern westernized countries, that pelvic organ prolapse has reached epidemic proportions. In the developing world, among squatting populations, these disorders are quite rare. ...African and Asian women seem to be relatively unaffected [by pelvic floor problems].36Prolapse appears to be comparatively uncommon in much of the developing world, despite the much greater multiparity of its mothers ...34 [Multiparity means having many children.]This evidence has baffled western doctors, since it contradicts their assumption that the pelvic floor is unsuited for bipeds. Their usual response is to claim that the problem is simply "underdiagnosed." Like the quadrupedal theory itself, this claim is asserted without any supporting evidence. For example, the last quotation goes on to say, "It is uncertain if this is a real difference; [women in the developing world] may merely complain less." But these women have to perform strenuous physical labor, just to survive. Daily chores include carrying buckets of water, tilling the fields, and washing clothes by hand. Pelvic hernias would make them virtual invalids. If they do not "complain" it can only mean that they do not dislodge their pelvic organs by the habitual use of the Valsalva Maneuver. Furthermore, no amount of stoicism could conceal the presence of incontinence, the other major sign of pelvic floor dysfunction. "Unavoidable" ailments mean job security, so gynecologists are quick to dismiss the possibility that "female troubles" can be prevented. Enormous amounts of money are at stake, creating an obvious conflict of interest. The average cost for a hysterectomy ranges from $7,000 to $16,800 ... the annual cost for hysterectomies in the U.S. exceeds $5 billion.26... the cost of surgical management of genital prolapse has surpassed $10 billion annually in the United States alone.36Fortunately, a few gynecologists have a more enlightened perspective. Dr. Stuart Stanton and Dr. Ajay Rane were quoted above, strongly advocating the squatting posture for pelvic health. Other physicians have deplored the harm done by their colleagues in performing unnecessary surgery. Richard W. Te Linde (1894-1989) was the editor of the standard textbook on gynecological surgery. He is quoted in the Spring 2004 Whole Woman Newsletter: ...in the practice of gynecology, one has ample opportunity to observe countless women who have been advised to have hysterectomies without proper indications...I am inclined to believe that the greatest single factor in promoting unnecessary hysterectomy is a lack of understanding of gynecologic pathology... A Case History  Dr. Akilah El, ND, PhD, is a naturopath with a deep understanding (and personal experience) of gynecologic pathology. In 1991, while still a student, she was diagnosed with cervical cancer and uterine fibroids. Ignoring the dire warnings of her gynecologist, she cured herself without the use of drugs, surgery or radiation. Dr. Akilah El, ND, PhD, is a naturopath with a deep understanding (and personal experience) of gynecologic pathology. In 1991, while still a student, she was diagnosed with cervical cancer and uterine fibroids. Ignoring the dire warnings of her gynecologist, she cured herself without the use of drugs, surgery or radiation.A key factor in her recovery was the adoption of the squatting posture for elimination. This relieved the pressure on the pelvic floor and allowed the pudendal nerve to repair itself. In this way, the pelvic organs were reconnected to the central nervous system – the energy and intelligence that protects us from disease.Dr. Akilah has repeatedly verified the effectiveness of this simple lifestyle change in helping her patients resolve gynecological ailments. The results have convinced her that "98% of all hysterectomies are unnecessary and dangerous." Dr. Akilah has summarized her program of self-cure in a tape called "Healing Our Womb - The Cause, Cure, and Prevention of Uterine Fibroids." top of page |
Sexual Dysfunction
The previous section described how the habitual use of sitting toilets depresses the pelvic floor and causes a "stretch injury" to the pudendal nerve. This injury has many potential consequences – including incontinence, prostate dysfunction and chronic pelvic pain.A recent article in the American Journal of Obstetrics and Gynecology (May, 2005) described another common result: female sexual dysfunction. According to the researchers, this problem affects up to 43% of women in the United States. Reuters Health issued the following report: The explanation given in the gynecological disorders section above should help the doctors solve their "enigma." Once they understand the cause of pelvic floor nerve stretch injury, they can give their patients practical advice on preventing it.Even though the study only tested women, a man's pelvic floor is also vulnerable, as explained in the prostate disorders section. Nerve damage is the most likely cause of male sexual dysfunction, as well.Fortunately, damaged nerves can grow back when they are no longer subjected to daily abuse. By repairing the connection between the pelvis and the brain, one has a chance of regaining normal sexual function. top of page |
He quotes Dr. Henry L. Bockus, the author of the standard textbook, Gastro-Enterology: ... The ideal posture for [evacuation] is the squatting position, with the thighs flexed upon the abdomen. In this way the capacity of the abdominal cavity is greatly diminished and intra-abdominal pressure is increased, thus encouraging expulsion ...11Dr. Alexander Kira cites an article in the journal American Anthropologist and draws the following conclusion: We must bear in mind that while we regard the use of the water closet as natural, we represent only a relatively small percentage of the world's population, and a percentage that may be said, in an absolute sense, to be wrong, insofar as we have allowed civilization to interfere with our biological functioning.12Dr. William Welles, the chiropractor referred to above, wrote an article entitled "The Hidden Crime of the Porcelain Throne." Here is a brief excerpt: The design of the modern-day toilet was created with absolute disregard for the anatomy of the human body. On the conventional Western toilet, pressure is exerted inside the abdomen by pushing the diaphragm down in such a way as to push all the organs of the body downwards, causing them to sag (prolapsus), and creating dysfunction of the ileocecal valve. The abdominal muscles are left totally unsupported, as we have said, and the body suffers the consequences.Dr. Leonard Williams states that the modern toilet effectively paralyzes the abdominal muscles. "These muscles are little enough exercised by sedentary man, but when seated on the ordinary everyday water closet, he could not exercise them even if he would." 2top of page |
The results of this experiment have been clear and unequivocal. The experimental group has suffered dramatically higher rates of intestinal and urological disorders. The following diseases are almost exclusively confined to the Western World: appendicitis, colon cancer, prostate disorders, diverticulosis, bladder incontinence, hemorrhoids, and inflammatory bowel disease. But the results have been misinterpreted by researchers who were unaware that the experiment was even taking place. Western doctors have tried to blame these diseases on the "highly refined" western diet. Their attempts have consistently failed to show that diet is a significant factor. Conventional medical websites all tell the same story: This is a disease of the Western World. We don't know what causes it, or why the developing world seems so strangely immune.Medical researchers have been working diligently to solve these deadly mysteries, but they have made little progress. Due to their habit of studying diseases in isolation, they failed to notice a remarkable coincidence: Many different bowel, bladder and pelvic diseases – previously rare or unknown – suddenly became commonplace in the last half of the 19th century. This simple observation would have alerted them to the presence of a common underlying factor. It would have prompted the obvious question: What suddenly changed in the daily habits of the population? The obvious answer: They abandoned the squatting posture for bodily functions (including childbirth.) For each disease, the anatomical relevance of this change has been explained above. The relevance is confirmed by the absence of these disorders among squatting populations.In conclusion, the porcelain throne has caused enormous amounts of needless suffering, and the annual waste of billions of dollars in health-care costs. Clearly, the time has come to reacquaint Western Man with his natural habits – and put this unfortunate experiment to an end.top of page |

# # #
top of page |
Do-It-Yourself Earthing Device Nature's Platform 186 Westside Drive Boone, NC 28607, USA 828-297-7561 Email address: NaturesPlatform [AT] hotmail.com |
Return to Hemorrhoids
No comments:
Post a Comment